info@footandankleunit.co.za | +27 11 647 3735 | +27 11 485 1974 | +27 11 647 3435
PATHOLOGIES
ANKLE CONDITIONS
Posterior Ankle Impingement
What is it?
Posterior ankle impingement is a condition where soft tissue or bony structures at the back of the ankle become compressed (pinched) during movement, especially when the foot is pointed downwards (plantarflexion). This often leads to pain at the back of the ankle, particularly in activities like ballet, sprinting, or football that require repetitive plantarflexion.
It is frequently seen in athletes and dancers, but it can affect anyone who regularly loads the back of the ankle.
CAUSES
Posterior ankle impingement may be due to:
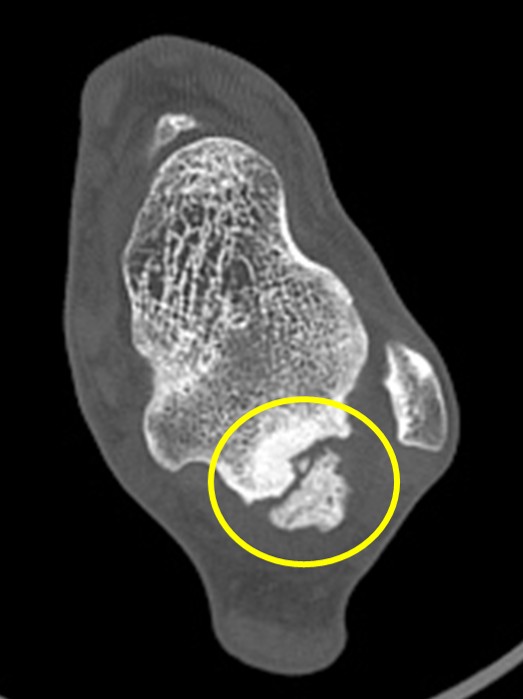
- Os trigonum: A small extra bone behind the talus (present in ~10–15% of people) that can get pinched.
- Prominent posterior talar process: An enlarged part of the talus (Stieda process) causing compression.
- Repetitive plantarflexion: Can cause inflammation of the soft tissues or irritate small bony areas.
- Previous injury: Especially ankle sprains, which may lead to scarring or instability that exacerbates impingement.
- Tendon entrapment: The flexor hallucis longus (FHL) tendon passes through the back of the ankle and can become irritated or trapped.
SYMPTOMS
- Deep, aching pain at the back of the ankle, worse during or after plantarflexion (e.g., pushing off, going down stairs, pointing toes).
- Swelling or tenderness at the posterior ankle.
- Clicking or catching sensation.
- Pain with forced plantarflexion tests (like ballet en pointe position).
- Pain may be intermittent or constant, depending on activity level.
DIAGNOSIS
Diagnosis is based on clinical examination and imaging:
- Physical exam: Tenderness behind the ankle, pain with forced plantarflexion, or FHL tendon irritation.
- X-rays: Can identify an os trigonum or enlarged talar process.
- MRI: Useful for evaluating soft tissue inflammation or FHL tenosynovitis.
- CT scan: Provides detailed bony anatomy if surgery is being considered.
- Ultrasound: May help evaluate dynamic tendon impingement.
TREATMENT OPTIONS
Non-Surgical:
- Activity modification: Avoid movements that provoke pain.
- Ice and NSAIDs: To reduce inflammation and manage pain.
- Physiotherapy: Stretching, strengthening, and improving ankle mechanics.
- Immobilisation (short period): In acute cases to allow inflammation to settle.
- Corticosteroid injection: May be used around the os trigonum or FHL sheath for diagnostic or therapeutic purposes.
Surgical:
Indicated if symptoms persist despite conservative management for 3–6 months, particularly in athletes.
- Posterior ankle arthroscopy (minimally invasive): To remove the os trigonum, debride scar tissue, or release the FHL tendon sheath.
- Open surgery: May be considered in more complex cases.
- Recovery: Typically allows return to sports within 3–4 months.
PROGNOSIS
- With appropriate treatment, most patients experience full resolution of symptoms.
- Early diagnosis and activity modification are key to avoiding chronic impingement or long-term dysfunction.
- Surgical outcomes are generally excellent, especially in athletic populations.